Built for the Wrong Disease
The healthcare system designed for acute illness is failing the chronic disease crisis and why the next line of professionals must fill the gap.

Originally written in the early days of COVID-19. Updated 2026 because the emergency passed, but the problem didn’t.
As I write this updated version, we are no longer in the middle of a world crisis. We are on the other side of one. COVID-19 has receded into the category of historical event, the kind of thing that gets a chapter in textbooks and a handful of retrospective documentaries. Hospitals are no longer triaging in parking lots. Ventilator counts are no longer daily headlines. Most people have genuinely moved on.
But here’s the thing about moving on: it doesn’t change the underlying math.
When I wrote the original version of this article in 2020, I was attempting to crystallize something I had been turning over in my head for years, a slow-moving collision between the healthcare system we have built and the population it is being asked to serve. COVID didn’t create that collision. It just forced everyone to look at it directly, for a moment, before looking away again.
I have spent most of my adult life working at the intersection of biomedical science, healthcare, technology, and entrepreneurship, whatever that means. Over the last several years, specifically, I have been actively building technology, businesses, and education platforms around how we can better address the health crises that currently impact our society and that are the inevitable consequences of the path we are on. Outside of set work hours, I spend much of my cognitive free time thinking about the future health of our species. This is not a hobby. It is, at this point, something closer to an obsession.
To quote Agent Smith in the Matrix: “I am inevitable.” We have marched down certain pathways of cause and effect, and we must begin thinking clearly and building systems to address the effects that are coming our way. The original article was my attempt to lay that out. This is the updated version, same architecture, current data, and one additional section I didn’t write the first time around, because in 2020 I was still focused on the problem. Now I want to talk about who fills the gap.
Part 1: The Burdening
In science and medicine, definitions are important, as is precision. So let’s begin with one.
Burden can be a noun or a verb. As a noun, it is something that is carried, a load, a duty, a responsibility. As a verb, it means to load heavily, or to cause someone hardship or distress. The general thesis here is that the burden being placed on the healthcare systems in the United States, and in the world at large, is unsustainable. Furthermore, the healthcare system as it currently exists is being asked to address problems it was not designed to solve.
To fully address this I want to break it down into several parts based on first principles: the current capacity of the U.S. healthcare system, the health status of the U.S. population, and the economics of the U.S. healthcare system. Let’s take them in order.
Part 1.1: The Current Capacity of the U.S. Healthcare System
One of the more interesting things that resulted from COVID-19 is that people became acutely aware, probably for the first time, of what the actual capacity of our healthcare system looks like. The headline that circulated was: “There are only 1 million hospital beds in the entire country.” Unfortunately, that was only one piece of the story.
To understand the true capacity, we need to dig deeper. Hospitals are just one component of the healthcare system. In addition to hospitals, there are clinics (primary care), outpatient care centers (urgent care), and specialized care centers (nursing homes, psychiatric care, birthing centers). Here is the current high-level picture:
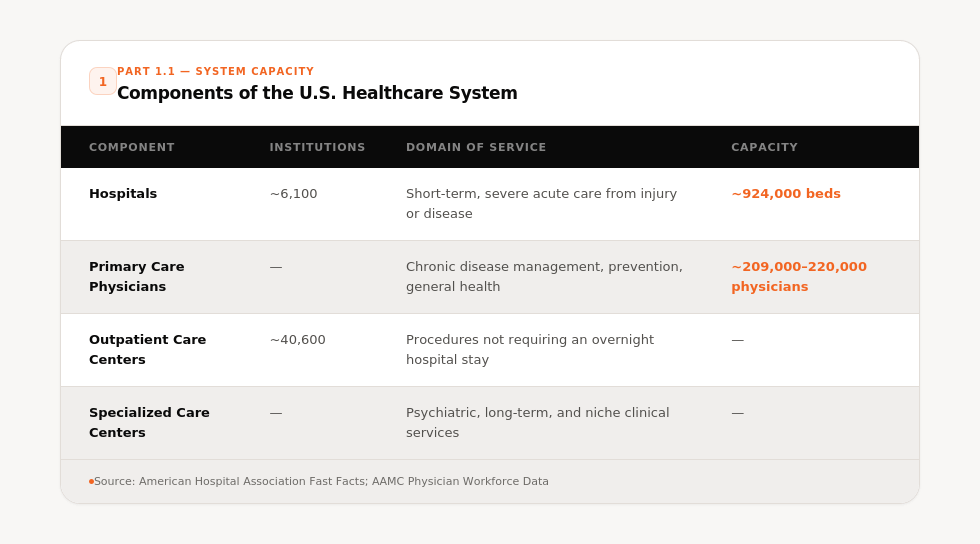
These numbers haven’t changed dramatically since 2020. What has changed is our understanding of how thin the margins really are and how much thinner they are getting.
Part 1.1.2: Hospitals and Carrying Capacity
Hospitals were created to serve a very specific function. They were built to provide short-term care for people with severe health issues arising from injury or disease. That is what they are optimized for. That is what they do well.
The distribution of hospitals across the U.S. is dominated by community hospitals, which make up the vast majority, roughly 5,100 of the ~6,100 total. Non-profit community hospitals account for more than 50% of that total. The number of hospitals has actually been declining since the 1970s, not growing, driven largely by consolidation and economics.
Now let’s look at what’s inside those hospitals, because this is where things get sobering.
There are approximately 924,000 total hospital beds in the U.S. Of those, about 790,000 are in community hospitals. Of those, approximately 107,000 are ICU beds. Breaking down the ICU beds further:
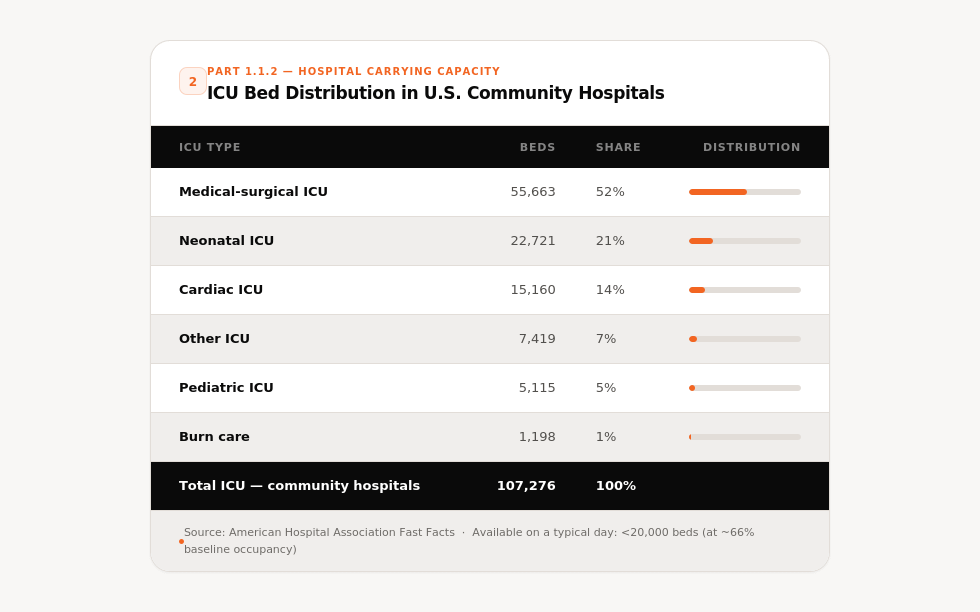
Here’s the perspective check. I live in the suburbs of Spokane, Washington, not a major city. The greater metro area has a population of about 520,000 people. In the event of a major health crisis requiring intensive care, we have enough ICU capacity in this country to handle roughly 20% of a metropolitan area that doesn’t even crack the top 100 in the U.S. That should stop you for a moment.
It gets more uncomfortable. The average hospital occupancy rate since 2000 runs roughly 66%. That means at any given time, of the ~924,000 hospital beds in the country, about 616,000 are occupied and only 304,000 are available. ICUs tend to run at even higher occupancy, and on a normal day there are likely fewer than 20,000 ICU beds available for a country of 340 million people.
What COVID revealed, what I was trying to articulate before COVID made it viscerally obvious, is that the carrying capacity of our hospital system works well for handling predictable, steady-state acute illness. It breaks under population-scale surges. If you took just 6% of the New York Metro population at peak COVID, you would fill every hospital bed in the country. Just 0.05% of that population would fill every ICU bed.
That is not a solvable problem by building more hospitals. Community hospitals cannot be architected to handle 10x or 20x surge events. The economics simply don’t work. This is a structural reality, not a policy failure, and it points to something more important: the solution to the chronic disease burden cannot be found inside hospital walls.
Part 1.1.3: Primary Care
Taking a significant liberty to oversimplify: if hospitals represent the acute care arm of the system, primary care represents the chronic disease management arm. Primary care physicians carry the theoretical responsibility for the ongoing health of the population, prevention, early detection, chronic disease management, the whole longitudinal arc of a person’s health over a lifetime.
As of the data we have, between 209,000 and 220,000 primary care physicians practice in the United States. That works out to roughly one primary care physician for every 1,500 Americans. In practice, given that physicians see an average of 16 to 17 patients per day and carry patient panels of around 2,200, the system processes approximately 460 million primary care visits per year, a number that grows as the population ages and the chronic disease burden expands.
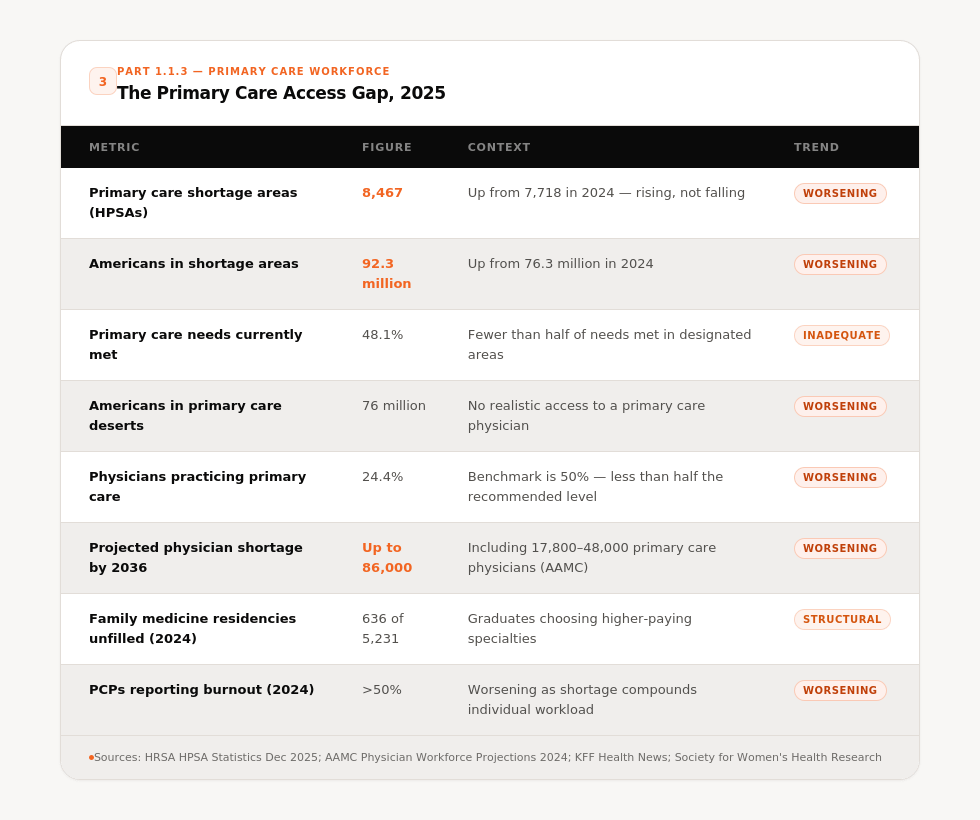
The gap between supply and demand here is not a projection anymore. It is happening now. The number of designated primary care Health Professional Shortage Areas rose from 7,718 in 2024 to 8,467 in 2025, and the population covered by those designations increased from about 76.3 million to 92.3 million. The AAMC projects a shortage of up to 86,000 physicians by 2036, including between 17,800 and 48,000 in primary care specifically.
The experiment of “just train more doctors” has been running for a decade and it is not panning out. More physicians enroll in medical school than ever before. New medical schools open every year. And yet: in 2024, family medicine programs left 636 residency positions unfilled out of 5,231 as students chased higher-paying specialties. CBS News Only 24.4% of U.S. physicians currently practice in primary care, well below the accepted benchmark of 50%. ChenMed Harvard, Yale, and Johns Hopkins don’t even have full family medicine departments. If you are a medical student at an elite institution and you show interest in primary care, you are still, in 2025, likely to hear from peers and professors: if you’re so smart, why would you choose that?
The structural incentive problem is not going away. And even if it were solved tomorrow, training a physician takes a decade. The demand curve is not going to wait.
Part 1.2: The Health Status of the United States
Let’s start with the broadest number and work inward.
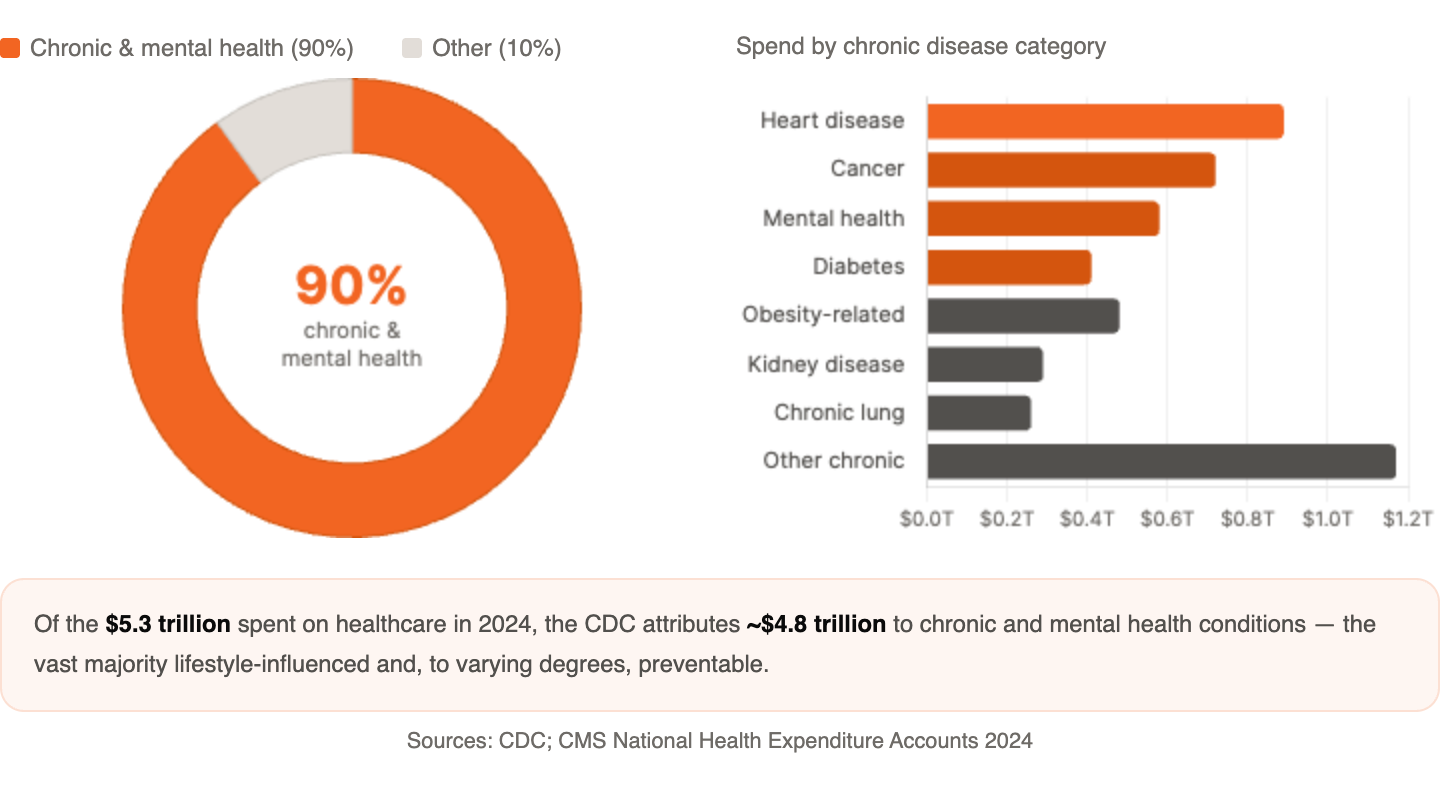
The United States spent $5.3 trillion on healthcare in 2024, $15,474 per person, accounting for 18% of GDP. CMS When I first wrote this article, the number was $3.5 trillion and I called it staggering. It has grown by $1.8 trillion in roughly five years. From a modest 5% of GDP in 1960, it rose to 13.3% by 2000 and has continued its upward trend to reach the current 18%, a growth trajectory that far outpaces other developed nations and leaves the United States with the highest health spending as a GDP share among OECD countries. Statista Projections carry that number to 20.3% of GDP by 2033.
According to the CDC, 90% of that cost is attributable to chronic and mental health conditions. The leading chronic diseases in the United States are heart disease, cancer, diabetes, and kidney disease, and obesity sits underneath most of them as the primary modifiable risk factor.
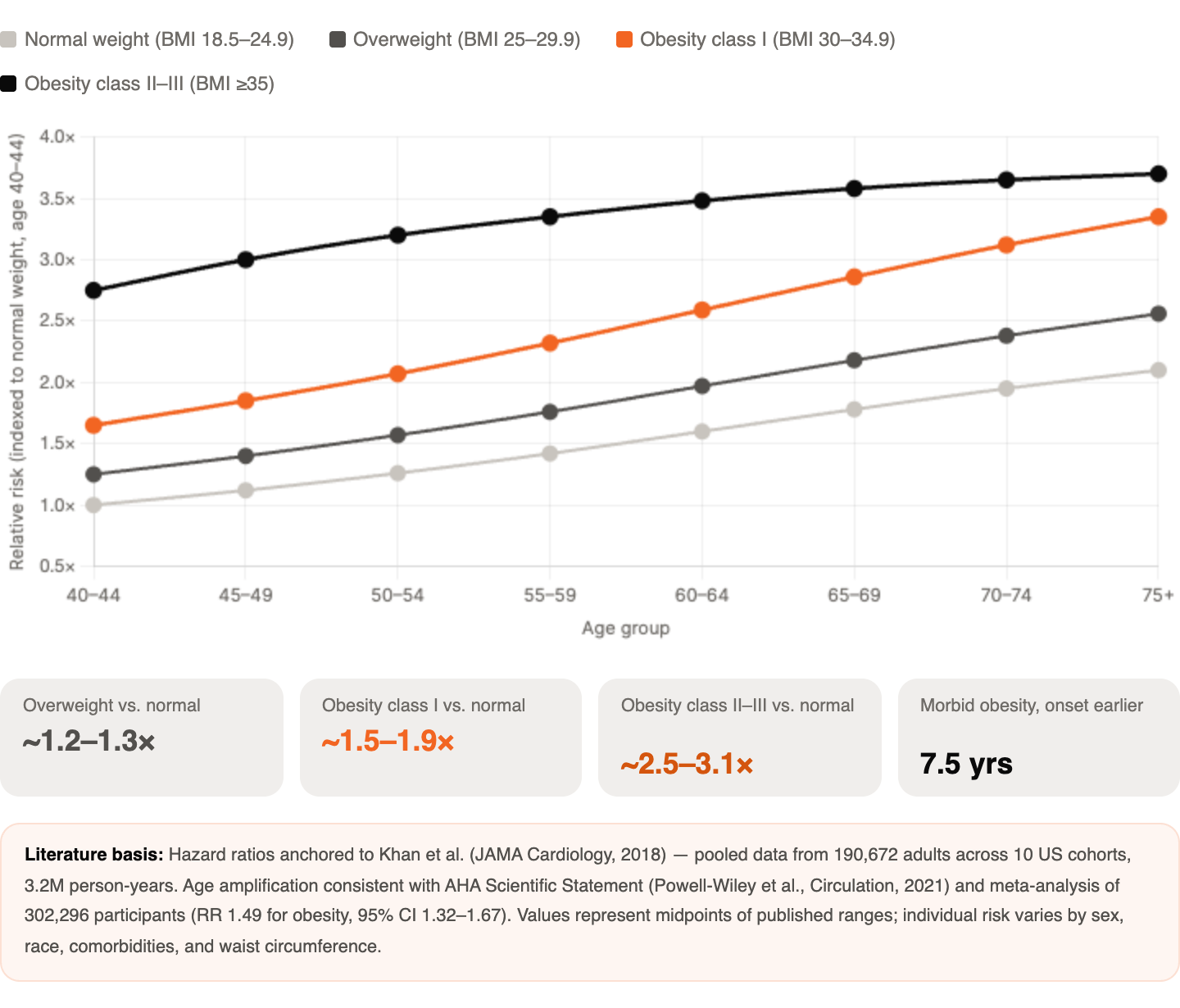
The relative risk data on this is worth dwelling on. In some populations, the relative risk of cardiovascular disease runs roughly 1.2 in individuals who are overweight and 1.5 in individuals with obesity. The relative risk of diabetes runs roughly 1.5 in individuals who are overweight, 2.5 in those with obesity, 3.5 in class II obesity, and 5.1 in class III obesity. One landmark study of roughly 100,000 people found that obesity reduced the number of disease-free years by approximately a decade, an effect greater than smoking, physical inactivity, and socioeconomic status combined, by a factor of two to four.
Part 1.2.1: The Obesity Picture in 2025
When I wrote the original article, the adult obesity rate in the U.S. sat at 42.4% and projections had us hitting 50% by 2030. The data since that time has told a more complicated story.
Current data places the adult obesity rate at approximately 40.3%, slightly lower than the peak but still higher than it was a decade ago. That modest plateau is real, but it comes with important caveats. The prevalence of severe obesity increased from 7.7% in 2013 to 2014 to 9.7% in 2021 to 2023, a 26% relative increase over the decade. - While overall rates may be leveling off, the severity distribution shifts in the wrong direction.
In 2024, all U.S. states and territories had an obesity prevalence of 25% or higher, with the Midwest at 35.9% and the South at 34.5% leading the nation. CDC Obesity rates are increasing among children and adolescents, with just over 21% of U.S. children and adolescents ages 2 to 19 having obesity, a rate that has more than tripled since the mid-1970s.
The thing I want you to sit with is this: the disease complications that arise from obesity lag behind the development of obesity. This happens for two reasons. First, most chronic disease develops through a lifetime accumulation of risk, and obesity acts as a magnifier and accelerant of that risk. Second, the diseases that follow obesity run on a physiological clock, type 2 diabetes developing over years and sometimes decades of smoldering subclinical pathology before it surfaces clinically. The same holds for cardiovascular disease, kidney disease, and much else.
This means that while we carry a substantial chronic disease burden today, we have not yet hit the peak. The obesity of 2010 is becoming the cardiovascular disease of 2025. The obesity of 2020 is becoming the disease of 2030 to 2035. Our population ages, obesity rates remain near historic highs, and the disease wave follows with a 7 to 12 year lag. We are watching a slow-motion surge build in real time.
Part 1.3: The Economics
This topic warrants a much longer treatment than I will give it here, but the summary matters.
Health spending totaled $74.1 billion in 1970. By 2000, health expenditures reached about $1.4 trillion, and by 2024 the amount spent on health more than tripled to nearly $5.3 trillion. Healthcare accounts for 24% of all government spending and stands as one of the largest categories of consumer spending. The rate at which healthcare consumes GDP has been one of the most consistent trends in American economics for sixty years, climbing from 5% in 1960 to 18% today, the greatest share of GDP in the entire world by a significant margin.
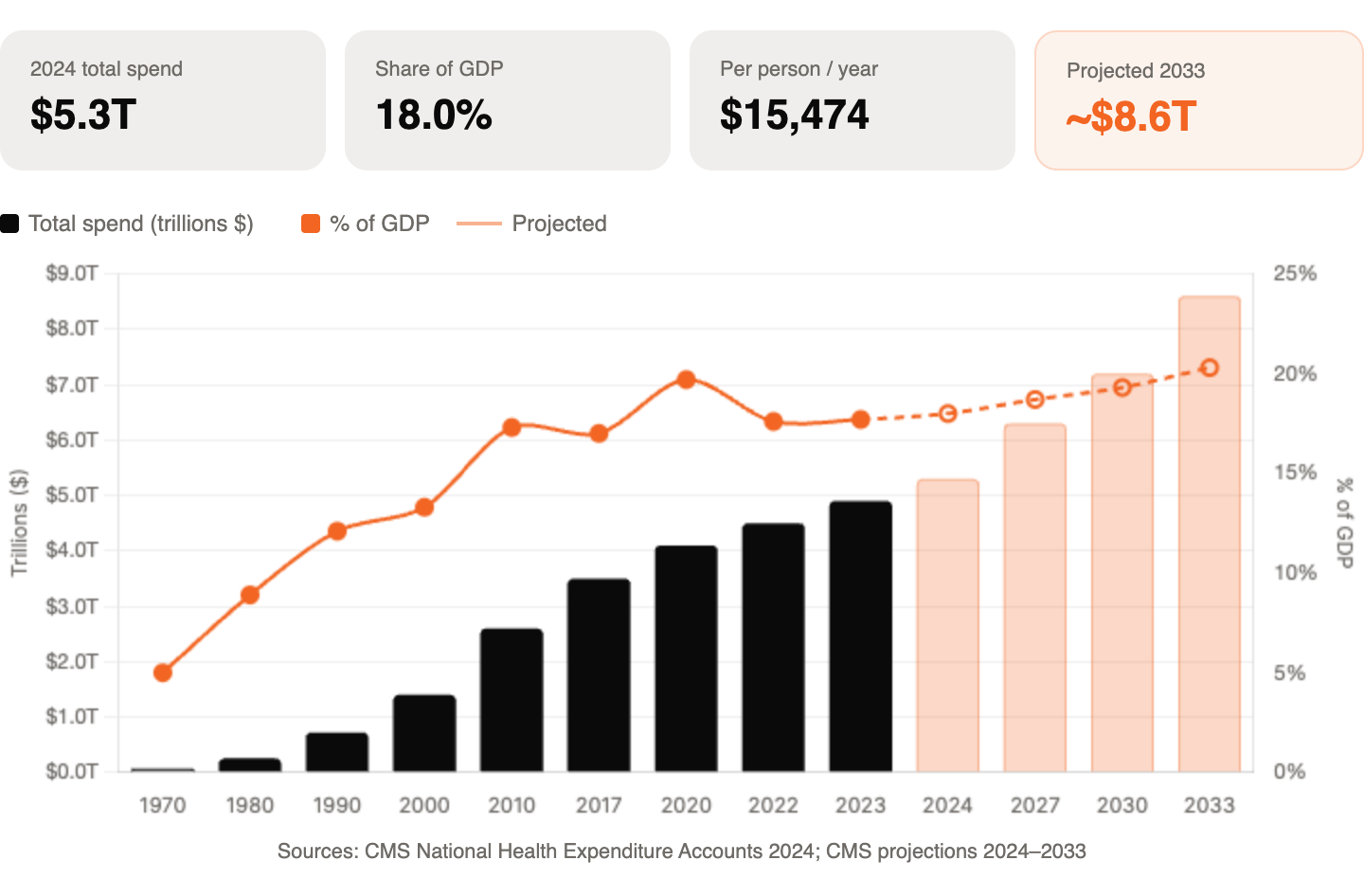
Over the 2024 to 2033 projection period, national healthcare expenditure growth averaging 5.8% is expected to outpace GDP growth averaging 4.3%, pushing the health share of GDP to 20.3% by 2033. We are heading, on current trajectory, toward a reality where one in five dollars generated by the entire American economy goes to managing disease. Most of it preventable. Nearly all of it chronic.
Part 1.4: Summary of Part 1
The current capacity of the healthcare system handles the predictable, steady acute medical care needs of the population reasonably well. It does not have the capacity, nor the design, to handle major surge events, as COVID made viscerally clear, nor to absorb the chronic disease burden of an aging, metabolically burdened population over the coming decades.
We have a growing and aging population, a population carrying high and entrenched chronic disease burden, and a disease wave building behind two decades of rising obesity. The physician pipeline will not solve this. Training more doctors does not fit the timeline of a problem that arrives faster than physicians can be produced. And even if it did, the physician model as currently structured, 15-minute appointments, volume-based incentives, reactive rather than preventive, reaches for the wrong tool.
The economic math points toward 20 to 25% of GDP going to disease management within the next decade. That number should prompt every person in or adjacent to healthcare to ask one serious question: is this sustainable, and if not, what changes?
Part 2: Of Powderkegs and Risk Escalation
The COVID crisis offered an opportunity to see our situation with unusual clarity. I want to revisit that framing because while the acute emergency has resolved, the structural conditions that made it dangerous remain fully intact.
Let’s review what we are actually dealing with.
The population that filled ICUs during COVID was not random. It was highly predictable. The individuals most likely to require intensive care, most likely to need ventilator support, most likely to die, were older adults with obesity, cardiovascular disease, diabetes, and chronic lung disease. Not because COVID singled those people out, but because those conditions had already spent years quietly degrading the physiological reserve those people needed to survive an acute respiratory insult. COVID was the spark. Chronic disease had been laying the kindling for decades.
This is the powderkeg, and it is important to understand what it is actually made of. The fuel is not insufficient ICU capacity, though that is real. The fuel is a population whose chronic disease burden has grown so large and so entrenched that any acute stress on the system, whether a novel pathogen, a natural disaster, or a bad flu season, cascades into a crisis because the baseline health of the population provides almost no buffer. We do not primarily have an ICU bed problem. We have a population health problem that shows up as an ICU bed problem when things go wrong.
Between 130 and 140 million Americans currently carry obesity. Roughly the same number carry established cardiovascular risk. About 37 million Americans have diagnosed diabetes and another 90 plus million have prediabetes. Tens of millions more carry chronic lung disease. These are not people who are one bad diagnosis away from needing a hospital. They are people who need better options for managing their health over the course of their lives, and right now the system offers them very few. The access points that exist are episodic and reactive. A physician visit every few months, a lab panel, a prescription renewal. There is no sustained infrastructure for the kind of longitudinal, behavioral, day-to-day support that actually moves the needle on chronic disease. And because that infrastructure does not exist, people do not know where to turn. They do not know what kind of professional can help them, what that help actually looks like, or how to find it. So they do nothing, or they cycle through the acute care system, using resources designed for episodic emergencies to manage conditions that are fundamentally chronic and longitudinal. The emergency department was not built to be the primary care setting for a diabetic patient who has no other access point. The ICU was not designed as the endpoint for a decade of unmanaged hypertension and metabolic disease. And yet that is increasingly what we are asking those institutions to do, not because patients are making bad choices, but because we have not given them better ones.
This is what I mean by risk escalation, transferring ownership of risk and accountability for that risk up the chain. Every year that we fail to meaningfully address the chronic disease burden at the lifestyle and behavior level, we push more of that risk upstream into the clinical system. Every year that primary care remains under-resourced and inaccessible, we push more of that risk further upstream into emergency and acute care. Every year that emergency and acute care absorbs demand it was not designed to handle, we edge closer to a system that breaks not because of a pandemic, but simply because the baseline load exceeds the design capacity.
COVID did not create this dynamic. It revealed it. And the uncomfortable truth is that building more ICU beds would not have fixed it. You cannot build your way out of a population health problem with acute care infrastructure. The math does not work, the economics do not work, and the timeline does not work. If we doubled ICU capacity tomorrow, we would fill it, because the population generating demand for that capacity is not shrinking. It is growing, aging, and accumulating more chronic disease burden every year.
The real intervention point is not downstream in the hospital. It is upstream in the daily lives of the population, in the choices, habits, environments, and support structures that determine whether a person arrives at sixty with metabolic resilience or with a decade of compounding chronic disease already on board. That is where the powderkeg gets defused. Not in the ICU.
Part 3: The Gap and Who Fills It
This section did not exist in the original article. In 2020 I was focused on describing the problem. In 2025 I want to talk about the solution, or at least the beginning of one.
Here is the central observation: an enormous gap exists between the physician’s office and the patient’s daily life. That gap is where the actual determinants of chronic disease live. It is where food choices happen, where movement habits form and erode, where sleep gets sacrificed and stress compounds. It is where a person either builds the physiological resilience to stay healthy for decades or gradually accumulates the risk that eventually surfaces in a clinical setting as a diagnosis.
Medicine has almost no presence in that gap. And that is not a failure of medicine. It is a recognition of what medicine was built to do. Physicians are trained to diagnose and treat disease. They are not trained, and do not have the time or the structural mandate, to coach people through the daily behavioral choices that would prevent disease in the first place.
So who does?
The answer that I keep coming back to, the one that the data, the economics, and the structural logic all point toward, is this: personal trainers, nutritionists, and health coaches are the next line of professionals that the healthcare system desperately needs and does not yet know how to use.
I want to be precise about this. I am not suggesting that a personal trainer replaces an endocrinologist or that a nutrition coach substitutes for a registered dietitian doing medical nutrition therapy. Scope of practice exists for important reasons and the lines should hold. What I am saying is different: the clinical system fails to occupy the space upstream of clinical disease, and the professionals best positioned to occupy that space are the ones already operating there.
Think about what a skilled personal trainer actually does. They meet a client where they are. They build a relationship over months and years. They understand that body composition, movement quality, and metabolic health are deeply intertwined. They provide accountability in a way that no 15-minute physician appointment ever can. They show up in the daily lived experience of the client in a way that no clinical professional does.
Think about what a skilled nutritionist or health coach does. They help people build habits that stick. They navigate the behavioral and psychological dimension of why people eat the way they eat and live the way they live, the dimension that medicine largely ignores because it does not fit neatly into a diagnosis code or a prescription pad.
National healthcare expenditure growth is expected to outpace GDP growth every year through 2033, pushing the health share of GDP to 20.3%. Health Affairs Most of that spending covers chronic disease. Most of chronic disease is lifestyle-influenced. The professionals with the deepest, most sustained access to lifestyle are not physicians. They are coaches and trainers.
The integration imperative is real. Some health systems have begun embedding health coaches in primary care settings. Lifestyle medicine as a formal specialty has grown substantially over the past decade. A handful of insurers are piloting reimbursement for coaching services tied to chronic disease outcomes. GLP-1 medications like semaglutide are generating genuine results in obesity, but a medication is not a behavior change. The evidence consistently shows that pharmacological and behavioral interventions work best in combination. The pill alone does not change the habits, the environment, or the lifestyle that generated the disease. The coach does.
The opportunity here for anyone operating in the fitness, nutrition, and wellness space is not incremental. It is structural. The healthcare system cannot solve the chronic disease problem from inside the clinic. The gap is real, it is enormous, and it waits to be filled by professionals with the right training, the right positioning, and the right integration with the clinical system.
Building the credentialing, the referral pathways, the outcome frameworks, the standards of practice that make that integration possible, that is the work of the next decade. It is also, I would argue, the most important work in health right now.
Closing
At this point it is important to step back and look at this from an event-agnostic perspective. The acute crisis of COVID has passed. The structural crisis it revealed has not. We have a healthcare system built for one thing being asked to do another. We have a population whose chronic disease burden grows faster than the clinical system can absorb it. We have a physician pipeline that cannot be built fast enough, and a financial model heading toward consuming a quarter of the entire American economy.
Risk escalation, kicking the can down the road, only works until you run out of road. Then you pick the can up at the end of it, all at once.
The next line of professionals is not a nice-to-have. It is a structural necessity. The personal trainers, nutritionists, and health coaches who understand the depth of this problem and position themselves accordingly are not filling a niche. They are filling a gap that medicine itself cannot close.